INTRODUCTION
Metastatic spinal cord compression (MSCC) is a common complication of metastatic disease, with high neurological morbidity [2]. Surgical decompression improves outcomes in selected patients, by preserving walking and sphincter function [4]. Anterior column decompression and reconstruction, supplemented with posterior fixation is the gold standard surgical treatment of MSCC when the tumour arises from the vertebral body. Surgical access to the anterior column has conventionally been through open lateral approaches. Open surgery is associated with pulmonary complications and may only be tolerated by patients who have better overall health scores.
The transpsoas extreme lateral interbody fusion (XLIF) approach is a minimally invasive procedure first described to gain access to the anterior column of the lumbar spine for the purposes of discectomy and interbody cage fusion [3]. This technique has been modified to allow for more extensive access across the thoracolumbar spine, and for addressing other pathologies affecting the anterior column [1]. The main advantage of this approach is that it is better tolerated by the patients, with fewer pulmonary complications.
We describe our 5-year experience with the surgical treatment of MSCC arising from the anterior column where vertebrectomy was indicated. Patients were managed with a modified direct lateral MIS approach procedure.
TECHNICAL NOTE
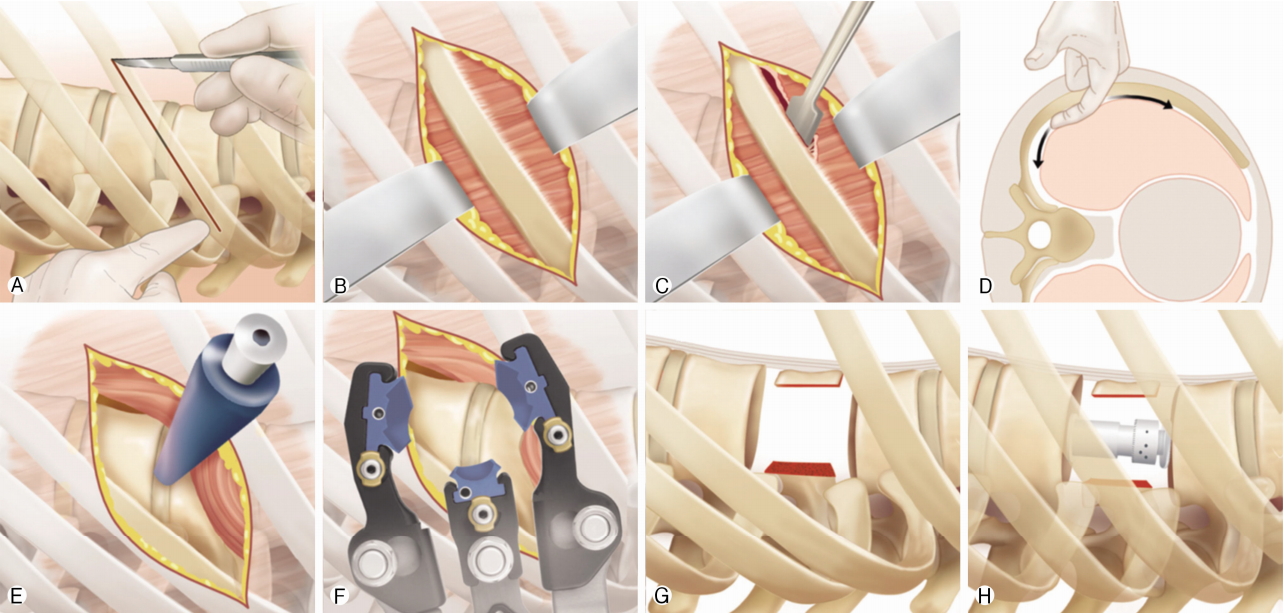
Double lumen ventilation is not required and the patient is ventilated normally throughout the majority of the procedure. This provides an immediate advantage over the open procedure where one lung is routinely collapsed. The patient is placed in the lateral position. A small incision is made over the rib overlying the vertebra of interest, determined by lateral image intensifier imaging (Fig. 1Ⓐ, Ⓑ). The plane between the superior surface of the rib and the intercostal muscles is developed both anteriorly and posteriorly by blunt dissection using the index finger alone, to allow for undermining and rib mobilisation (Fig. 1Ⓒ, Ⓓ). Momentum of the finger is necessary to strip the muscle off the superior aspect of the rib. Dissection with the finger is taken under the skin incision to as anterior as possible to the transverse process of the vertebra of interest, with care taken to minimise/avoid incursion through the pleura although in most cases the pleura is breeched (Fig. 1Ⓓ). If so, the ventilation is ceased and the lung is retracted with a Penfield or fingers and protected away from the anterior vertebral column and discs. A guidewire and dilators are placed between the ribs, under image intensifier with a temporary cessation of ventilation that typically lasts 2-3 minutes (Fig. 1Ⓔ, Ⓕ). The retractors are then slid over the dilators and are opened very gradually to allow rib displacement out of the surgical field. Lung tissue is protected by shims inserted within the retractor set to enable full ventilation. At the thoracolumbar junction the diaphragm insertions can be diathermied off the vertebral body. In the lumbar spine the retractors are placed transpsoas, and we recommend a primary ‘soft dock’ superficial to psoas to allow for direct visualisation and transposition of the nerves of the lumbosacral plexus.
At the end of the procedure the intercostal muscles overlying the rib are closed, with care taken to avoid injury to the neurovascular bundle underlying the rib. A purse string suture is placed and the anaesthetist induces hyperinflation in the patient prior to final closure to remove excess air from any pleural cavity defects. The patient requires close observation and chest radiography in recovery to ensure no residual large pneumothorax. No patients in this group needed an emergency placement of a chest drain in the postoperative period.
In our experience (JT) the advantage of this technique is that it is better tolerated by the patient. Firstly, there is optimal ventilation intraoperatively. Secondly there are smaller incisions with sparing of the rib and avoidance of chest drains, that contributes to earlier mobilisation and less post-operative pain.
MATERIALS AND METHODS
14 patients underwent this procedure from August 2012-August 2017.
Demographic and outcome data for selected patients was found from their electronic records on the Patent Pathway Manager (PPM), that included initial surgical assessment, dates of ward discharge and surgical and oncological follow up. The operation notes were found on the PPM in the format of a typed document (Bluespier). Surgical times were recorded on the Galaxy theatre operations system. The original clinical notes were pulled to provide further supporting information.
For each patient we identified demographic information, primary tumour histology, and surgery type including levels of surgery and supplementation with posterior decompression/fixation. Primary outcomes were estimated blood loss determined from operation note, duration of surgery, length of stay in high dependency unit and length of stay in the hospital. Secondary outcomes were procedure-related complications.
The patients were primarily operated by a single surgeon (JT), using a variety of lateral access retractors, including Nuvasive, Globus Medical and RTI Surgical products.
RESULTS
14 patients were identified undergoing the MIS approach. The demographic details and operations are listed in Table 1.
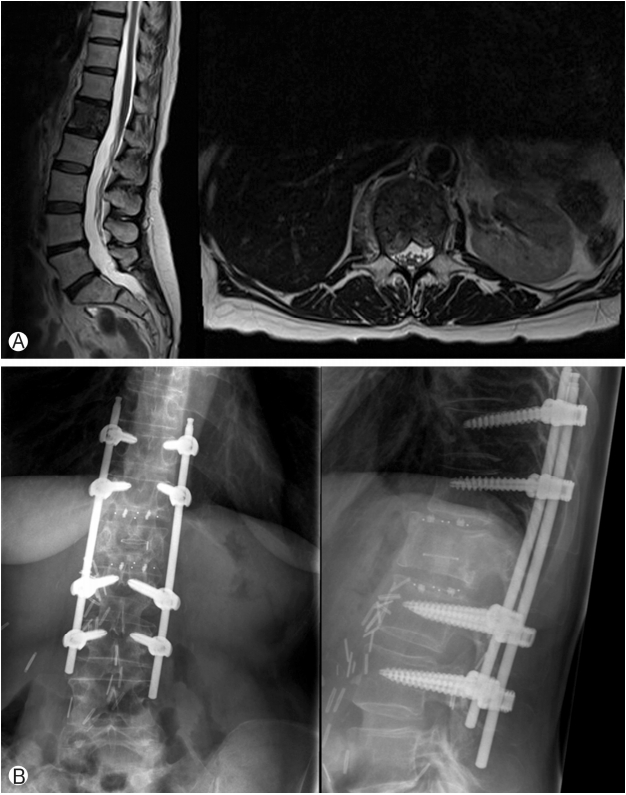
An example of the surgery is demonstrated in Figure 2 for patient 5.
10/14 patients underwent supplemental posterior fixation. These were a combination of open and percutaneous, with additional posterior decompressions in some cases where tumour was causing posterior compression as well. This was performed through a small midline laminectomy approach centred between the percutaneous pedicle screw fixation which was either one or two levels above and below the infiltrated vertebra.
The outcomes of the patients are shown in Table 2. 11/14 (79%) had less than 1 L blood loss during the procedure. The mean duration of the procedure was 5 hours 51 minutes. 5/14 (36%) avoided HDU, and the median duration of time spent in HDU was 1.5 days. 3 patients required a chest drain, but none as an emergency. The median length of stay in hospital was 16 days, and 4/14 (29%) were discharged within 1 week. There was 1 major complication requiring revision surgery although this was unrelated to the direct lateral approach. Patient 3 deteriorated neurologically post operatively due to an epidural haematoma that was evacuated. At the same time a pedicle screw position was modified for optimisation.
DISCUSSION
Surgical treatment of MSCC is challenging and high risk. Robust referral pathways are required locally to ensure rapid diagnosis and appropriate onwards referral with input from oncologists and spine surgeons, within a multi-disciplinary framework if possible as per NICE guidelines [5]. This clinical problem is increasing in frequency with an ageing population, better access to imaging and new oncological treatments. Surgical treatment remains the gold standard, and the advent of minimally invasive techniques opens the potential to provide surgical treatment to a wider group of patients.
We describe a novel technique of a rib sparing minimally invasive direct lateral approach to the thoracolumbar spine. This case series demonstrates that this approach is feasible and safe. There is typically a high risk of complications with these patients, reflecting the nature of the surgery and the underlying pathologies. In this case series there was only 1 major complication requiring revision surgery. There were 2 patients that required insertion of chest drains in the post-operative period, which was done in a controlled manner with no harm to the patients. We contend that patients do not require chest drains as standard, although they do require immediate post-operative chest radiography and close observation in the first 24 hours for evidence of respiratory compromise. All patients planned for the minimally invasive approach completed their vertebrectomy without removal of rib or formal thoracotomy. The only situation where we would anticipate difficulties with the rib sparing MIS approach would be where there is reduced chest compliance limiting rib distraction, such as patients with ankylosing spondylitis.
In summary we contend that minimally invasive vertebrectomy is feasible and safe, and potentially offers patients lower ‘impact’ surgical treatment. This can be applied to all pathologies including infection, trauma and degenerative disease. However, it is most applicable and beneficial in treating MSCC where patients are often frail with multi-organ involvement and poor physiological reserve. As oncological treatments improve and surgery becomes better tolerated, there is a case for a rethink of the role of surgery, which historically has been restricted to preserving neurological function in patients with reasonable oncological prognoses. In this series there are patients with very poor prognoses, where the role of surgery was to treat unremitting mechanical pain refractory to medical management rather than preservation of neurological function. As oncological medical treatments improve and evolve, there should be a corollary innovation in the role of surgical treatment and the form that it takes.