Percutaneous Endoscopic Lumbar Foraminoplasty for Resection of Synovial Cyst
Article information
Abstract
Synovial cyst is an extradural mass that compresses nerve root or thecal sac. Surgical excision with partial hemilaminectomy and medial facetectomy is commonly used for synovial cyst. Remarkable advancements in endoscopic spinal surgery have led to successful outcomes comparable to conventional open surgery. Here we introduce percutaneous endoscopic lumbar foraminoplasty for resecting synovial cyst as a minimal invasive technique. A 59-year-old woman presented with radicular pain at left L5 dermatome. Magnetic resonance images demonstrated a synovial cyst at left L4-5 facet joint and degenerative spondylolisthesis on L4-5. Under endoscopy, synovial cyst was removed by piecemeal method after transforaminal endoscopic foraminoplasty that removed part of superior facet. Her symptoms were relieved and the patient was discharged the next day. Therefore, percutaneous endoscopic lumbar foraminoplasty can be used as a minimally invasive surgical option for synovial cyst. It may provide less traumatization and affect less postoperative instability.
INTRODUCTION
Synovial cyst compressing nerve root was first reported in 1950 [24]. Synovial cyst of facet joint can cause radicular pain and neurogenic claudication [5,19]. Unresponsive to conservative treatment, surgical removal is regarded as a definite treatment for persistent radicular pain or neurologic deficit. Whether additional fusion is necessary remains controversial. Remarkable advancements in endoscopic techniques and instrumentation have led to successful outcomes comparable to conventional open surgery [1,8,17,20]. Recently, several minimal invasive techniques including micro-endoscopic assisted approach and percutaneous interlaminar approach have been applied to remove synovial cyst [13,16]. Here we introduce percutaneous endoscopic lumbar foraminoplasty for resecting synovial cyst in the spinal canal as a minimal invasive technique.
CASE REPORT
A 59-year-old woman presented with radicular pain in the left leg from buttock to the lateral of thigh and leg. There was objective weakness of the great-toe dorsiflexion. On manual muscle test, it was graded as 4. Radiography (Fig. 1A) showed grade 1 degenerative spondylolisthesis at L4-5. Magnetic resonance (MR) images (Fig. 1B and 1C) showed synovial cyst at left L4-5 facet joint compressing the neural structures in the spinal canal. Computed tomography (Fig. 1D) showed round mass juxta at left facet joint. The radiating pain sustained after epidural steroid injection. Therefore, we planned cyst removal with endoscopic technique.
Lateral Radiography Ⓐ showing grade I spondylolisthesis. Magnetic Resonance (MR) images (Ⓑ, Ⓒ) showing synovial cyst compressing the thecal sac. Computed tomography Ⓓ showing well-demarcated round mass juxta facet joint.
This procedure was performed under local anesthesia with the patient lying in the prone position. The skin entry point was 13 cm from the midline at L4-5 disc space. After infiltrating the entry point with local anesthetics, an 18-gauge spinal needle was introduced under the guidance of fluoroscopic imaging. The target point of the spinal needle was the medial pedicular line on the anteroposterior image and the posterior vertebral line on the lateral image. Subsequently, an epidurography was performed using contrast media to confirm the location of the exiting and the traversing root. The following steps were then performed: a guide wire was inserted through the spinal needle; the spinal needle was removed; a small incision was made in the skin at the entry site; a tapered cannulated obturator was inserted along the guide wire. When the obturator touched the annulus, a bevel-ended working cannula was inserted along the obturator. The cannula was located outside the foramen and lateral border of the facet joint. The superior part of facet joint was removed by endoscopic drill (Primado 2, Nakanishi inc, Japan) (Fig. 2A). From outside foramen to inside foramen, partial part of the facet joint and foraminal ligament were removed by a drill, a cutting forcep, and an endoscopic kerrison punch. While engaging working cannula to the medial foraminal zone to undercut the superior facet and remove yellow ligament, white-yellowish mass (Fig. 2B) was encountered. With meticulous bleeding control, the mass was removed by piecemeal. After removing the mass, neural structures were released (Fig. 2C). After the procedure, the pain was improved. Postoperative MR image revealed complete removal of synovial cyst (Fig. 3). The patient was discharged the next day.
In the endoscopic view, partial part of superior facet (▲) was removed with endoscopic diamond drill Ⓐ. After removing the superior facet, yellowish mass (◆) was encountered, which was synovial cyst Ⓑ. After removing the mass with piecemeal method, neural structure (★) was found Ⓒ.
Postoperative axial Ⓐ and parasagittal Ⓑ MR images showing the removal of synovial cyst with partial removal of the superior facet.
DISCUSSION
Synovial cyst is an extradural mass that compresses nerve root or thecal sac [5,19]. Synovial cyst usually presents radiculopathy. It can also cause neurogenic claudication with pre-existing spinal stenosis [12,18]. It is associated with degenerative changes, causing fluid extrusion from the joint capsule. It is commonly found in spondylolisthesis, osteoarthritis, and disc degeneration in the mid- 60s [4]. The incidence of synovial cyst is reported to be 2.3% [10,22]. L4-5 level is the most affected segment [5]. It might be associated with mobility at that level. The natural history of the synovial cyst is not well established. Conservative treatments for synovial cysts have been reported to be less effective [6]. Percutaneous aspiration of the cyst also has higher recurrence and failure rates [11]. Surgical excision with partial hemilaminectomy and medial facetectomy is a common procedure for synovial cyst. Decompression alone can achieve successful results. For example, Lyon et al. have achieved 91% of good outcomes in 134 patients [18]. According to literature, cystic recurrence rate is about 2% after decompression alone [5]. However, recurrent back pain occurs in 20% of cases during the follow-up. It may be caused by segmental instability, hypermobility, and progression of degenerative changes. Extensive bone removal is associated with postoperative instability [21]. For spondylolisthesis after open excision, fusion surgery is required for 1.8% to 6% of patients [3,4,18]. Whether fusion surgery has better outcome than decompression alone remains controversial although fusion surgery decreases recurrent back pain [14,25]. Minimal invasive techniques for synovial cyst include micro-endoscopic assisted cyst removal, contralateral approach preserving facet joint, and endoscopic interlaminar approach [2,13,16]. Komp et al. have reported successful results of full-endoscopic synovial cyst removal [16]. They have solved synovial cyst in the spinal canal with interlaminar approach as in conventional posterior approach. Transforaminal approach is applied only to foraminal/extraforaminal synovial cyst. Epidural scarring can be reduced in endoscopic techniques based on postoperative MR images and revision surgery.
Knight et al. [15] have introduced laser-assisted foraminoplasty to ablate foraminal ligament and osteophytes (Table 1). Foraminoplasty has been applied to down-migrated disc herniation or sequestrated disc to remove superior facet and partial pedicle [7,23]. L5-S1 disc herniation with high iliac crest needs foraminoplasty for engaging working cannula [9]. Ahn et al. [1] have reported endoscopic foraminotomy for foraminal stenosis using an endoscopic drill, a side-firing laser, and a micropunch. This technique enables the visualization and the mobilization of both traversing nerve root and exiting nerve root under endoscopy to remove foraminal ligament, superior facet, and herniated disc. In this case, we were concerned that the posterior approach might require wide bone removal including large laminectomy and medial facetectomy which might cause instability at the index level. Transforaminal endoscopic approach might make it safer to remove synovial cyst, thus preserving facet joint as much as possible. Under endoscopy, it is safe to remove adequate bone and synovial cyst using an endoscopic diamond drill and endoscopic instruments. Furthermore, the transforaminal endoscopic approach is advantageous in that synovial cyst can be removed without needing the manipulation of neural structures. It might be able to reduce surgery-induced segmental instability. Theoretically, it has several drawbacks such as steep learning curve, results depending on surgeon, uncertainty of sufficient decompression, and difficulty in suturing a dural tear.
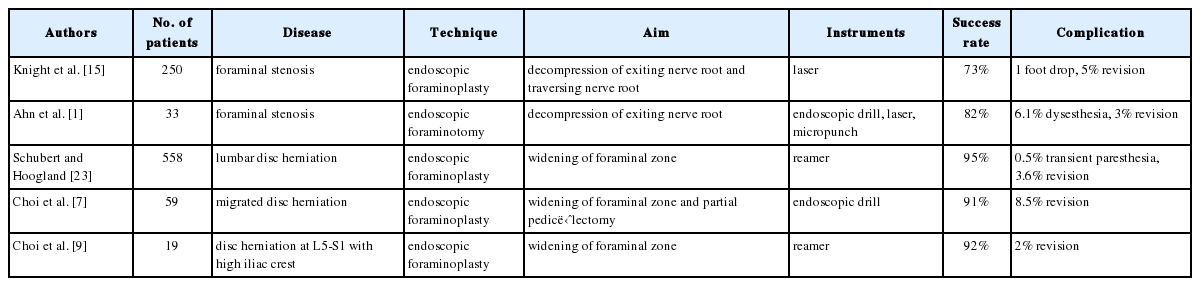
Clinical results of endoscopic foraminoplasty
CONCLUSION
Percutaneous endoscopic lumbar foraminoplasty can be used as a minimally invasive surgical option for synovial cyst. It may provide less traumatization and affect less postoperative instability.