Robotic-assisted Superior Gluteal Nerve Tumour Resection
Article information
Abstract
Sciatic notch tumours of the intra-pelvic variety are rare lesions and commonly arise from the sciatic nerve. These are usually benign neurogenic tumours and the most common of them is schwannoma. Conventional laparotomy techniques have associated surgical morbidity and significant blood loss. The advent of robotic systems and refinement in robotic-assisted surgical techniques to access deep lying pre-sacral lesions has offered a novel way to surgically handle such lesions thereby reducing morbidity, hospital stay and blood loss. Here we are presenting a case of non-discogenic sciatica which was attributed to superior gluteal nerve tumour and was surgically resected using robotic-assisted technique.
INTRODUCTION
The evolution of robotic-assisted surgery has been a boon to minimally invasive surgery. Since the first use of robotics based on laparoscopic principles in cardiothoracic surgery [1], many other specialities have taken the advantage of robotic systems. It has made surgically difficult cases more accessible and with less damage to the surrounding tissues.
Primary tumours of the superior gluteal nerve are unheard of Pre-sacral and sciatic notch tumours are uncommon cause of non-discogenic sciatic pain in the adult population and usually arise from the sciatic nerve [2]. Schwannomas are the commonest benign tumours in this anatomical location [3].
CASE REPORT
A 64-year-old lady presented with chief complaints of right buttock and radiating leg pain of one month duration. There was no history of injury or any other significant precipitating factor. The pain was insidious in onset, progressive, radiating, severe with paroxysmal severe pain (VAS 7–8). The pain distribution was along the S1 dermatome. There was no history of claudication and sensory loss or motor weakness. Bowel and bladder habits of the patient were normal.
Patient has a past medical history of hypertension, angina and hypothyroidism for which she is on medication. She has a past surgical history of hysterectomy 20 yours ago and L4–5 spine stabilisation in 2009. There is no other significant contributory medical history.
On clinical examination, the only finding was right buttock and posterior thigh paresthesia corresponding to S1 dermatome. Straight leg raising (SLR) test was negative. There was no sensory or motor deficit. DTR were normal. The patient was evaluated with standard pelvis radiographs (Figure 1), CT scan (Figure 2) and MRI scan (Figure 3) which revealed a mass in the right superior gluteal nerve.

Plain radiograph: L4–5 level reveals metal implants for posterior stabilization.
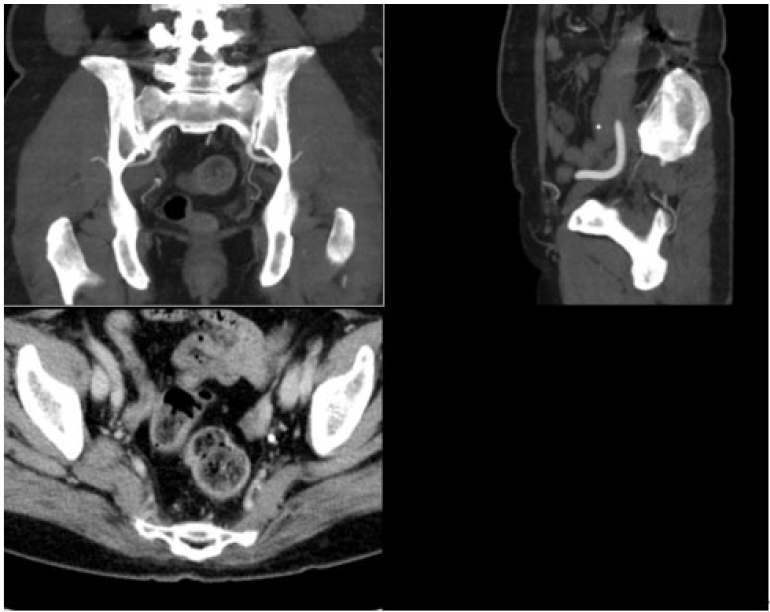
CT scan: Non-specific features of a mass lesion. No bony erosion.
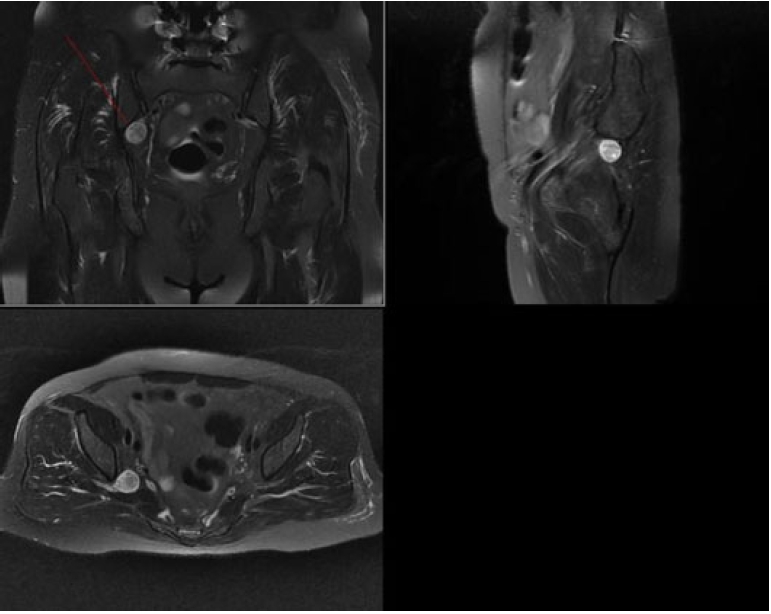
MRI scan: 2.4 cm lesion, isointense on T1 hyperintense on T2 and contrast enhancement, arising from the right superior gluteal nerve.
Except L4–5 level pedicle stabilisation implants no other feature was visible on plain radiographs.
CT scan images showed non-specific features of the mass, no bony lesion and contrast enhancement. MRI scan showed a 2.4 cm lesion, isointense on T1 imaging and hyperintense on T2 imaging and contrast enhancement, suggesting a neurogenic tumour arising from the right superior gluteal nerve. The symptoms were most probably due to pressure effect on the sciatic nerve at the sciatic notch.
1. Surgical Technique
The patient underwent pre-operative evaluation for surgical fitness.
Patient was operated under general anaesthesia with endotracheal intubation in supine lithotomy position (Allen chair). Foleys urinary catheter and rectal tube were inserted.
Patient was prepared, painted and sterile draping was done. Operated with Da Vinci Xi System. Total six surgical ports including 4 for robotic arms were used.
A small incision was made just below the umbilicus, CO2 gas is inflated up to 15 mmHg pressure to create pneumoperitoneum. Additional ports were made. After ruling out intestinal injury, the robotic system was docked. Trans-peritoneal route was used to approach right side retroperitoneal pre-sacral space close to the intra-pelvic portion of the sacral nerves close to the right internal iliac artery. Meticulous dissection was done, smaller vessels were cauterized and bisected. Tumour approached, resected and collected in retrieval bag (Supplementary Video; which demonstrates the procedure of surgery). Peritoneum closed in layers over drain. Scarring due to previous hysterectomy did not create any difficulty in surgical dissection.
Total blood loss of approximately 50 mL.
Duration of anesthesia: 170 minutes.
Duration of surgery: 135 minutes.
2. Histopathology Report
An irregularly shaped pale brown tissue specimen measuring 2.2×2.1×1.6 cm. Microscopic examination confirmed as schwannoma (Figure 4).
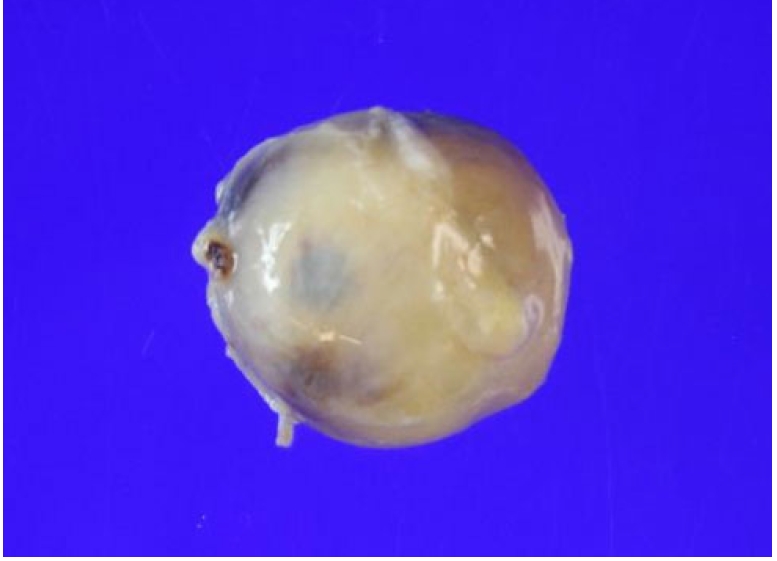
Gross features of the excised tumour mass.
3. Postoperative Scans
Postoperative MRI scan (Figure 5) showed resection of the mass and minimal fluid collection.
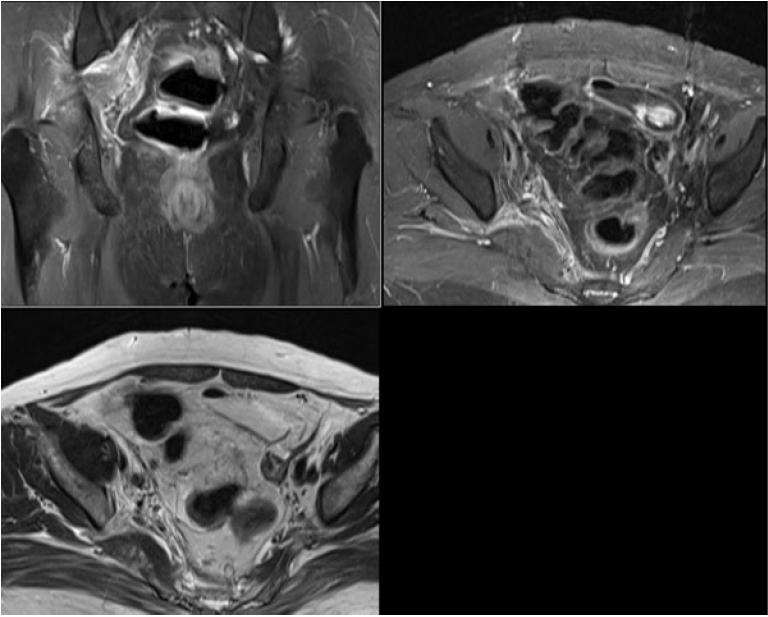
Post op MRI scan: Complete resection of mass.
4. Postoperative Patient Status
Patient was relieved of her symptoms postoperatively.
5. Review of Literature
The da Vinci surgical system was launched in 2014 as an improved version to da Vinci Si surgical system. It is currently in its 4th generation and is the most commonly used system for robotic-assisted laparoscopic surgery [4,5]. The da Vinci Xi Surgical system had improved features as compared to the previous generation machine with improved robotic arms, camera docking, longer instruments, new vision architecture and various other enhanced upgradations [4,6,7].
The superior gluteal nerve arises from the sacral plexus from the ventral divisions of L4, L5, and S1. It forms within the pelvis and exits through the greater sciatic notch superior to the piriformis muscle (suprapiriformis foramina) and divides into superior and inferior branches. It is a pure motor nerve. The superior gluteal nerve is accompanied by the superior gluteal vessels. This complex has an intrapelvic and an extra-pelvic course. The superior gluteal artery is the largest branch of the internal iliac artery whereas the superior gluteal veins are the venae comitantes to this artery [8,9].
Peripheral nerve root tumours are rare lesions with an estimated incidence of 1 in 100,000 [10]. Most common of these are benign schwannomas which are slow growing tumours [11]. 13.5% of peripheral schwannomas are reported in the lower limbs with sciatic nerve accounting for one percent cases. These tumours being slow growing have a thick capsule and hence complete surgical resection is possible and is the treatment of choice [12]. Schwannoma or neurinoma or neurilemmoma is a benign peripheral nerve tumour arising from Schwann’s cells [2]. These are the most common nerve root tumours. They occur in the age group of 30 to 50 years, with no specific gender predisposition. They may be solitary or multiple. Malignant transformation is rare. Sciatic notch schwannomas can be intra-pelvic, extra-pelvic or mixed type [3].
DISCUSSION
Sciatic notch tumours of the extra-pelvic type are approached through the infra-gluteal approach [13] or trans-gluteal approach [14], those of intra-pelvic type need a trans-abdominal approach [15] and dumbbell shaped lesions across traversing across the sciatic notch require a combined approach [14-16]. Reports of intra-pelvic lesions resected by the infra-gluteal approach [3] and extra-pelvic lesions resected using tubular retractor [12] have also been described.
The case presented here is purely intra-pelvic type. Tumours arising from the sciatic nerve or its branches near the sciatic notch have been described in the literature earlier [2,3,12,14,15]. One case arising from the pudendal nerve has been mentioned [17,18]. However, to our knowledge no case has been reported arising from the superior gluteal nerve.
Conventional trans-peritoneal or retro-peritoneal approach for intra-pelvic and dumbbell shaped lesions through a midline laparotomy cause significant surgical trauma and associated with complications related to the alimentary system, urinary system and encounters major blood vessels and nerves in the surgical field [3]. These procedures are associated with increased surgical time, high blood loss, increased stay in hospital and significant morbidity and mortality [14]. This approach is unavoidable in cases of large sized tumours, malignancies with or without surrounding infiltration, and in cases where lymph nodes involvement must be assessed or addressed. However, in benign lesions with relatively small size, the morbidity and mortality associated with the traditional approach are more problematic as compared to the symptoms.
Laparoscopic approach to pre-sacral tumours are also described but difficulty in visualisation, limited field of vision, restricted field for instruments and high complication rate make it a cumbersome approach [19,20].
In general, treatment for benign tours is en-bloc resection. However, radiosurgery can be performed when it is difficult to completely remove with surgical treatment or when there are many major structures around the tumour, so there is a high possibility of blood loss or nerve injury during surgery. If complications can be minimized and the tumours can be completely removed, surgical treatment is better than radiosurgery.
So, robotic-assisted technique provide a safe surgical option for resection of such benign tumours reducing the surgical time, blood loss and minimising the associated morbidity and mortality [21,22].
The price and installation of these systems, maintenance cost, training investment and reproducibility of good results with challenging surgical cases remains a major limiting factor in the use of these hi-tech surgical gadgets. Also, the availability of these systems is restricted to large multi-speciality centres.
CONCLUSION
Robotic-assisted nerve root tumour excision in the sciatic notch, especially of the intra-pelvic and mixed type, is an effective way for reducing surgical morbidity and blood loss as compared to conventional laparotomy techniques.
Notes
Ethical statements
This study has been approved by the institutional review board of Seoul Saint Mary's Hospital, Catholic university of Korea (KC22ZISI0296).
Conflicts of interest
No potential conflict of interest relevant to this article.