Post Herpetic Neuropathy of Sinuvertebral Nerve: A Case Report
Article information
Abstract
Varicella-Zoster virus is a neurotropic virus of the herpes virus family that primarily affects sensory nerves. Herpes zoster causing sinuvertebral neuropathy has not been mentioned in the literature. A 55 years old man presented with low back pain, both buttocks, posterior thigh and leg pain over last 3 months. A straight leg raising test was positive on both sides. A left great toe dorsiflexion was decreased to 4/5. The VAS score at admission for back and leg pain was 7/10. The patient MRI was showing disc degeneration at L5-S1 level. We performed endoscopic interlaminar annuloplasty using radiofrequency ablation to denervate the sinuvertebral nerve attached to the annulus under epidural anesthesia. Patient symptoms completely relieved at the postoperative period and continued upto recent follow up of 6 months. The classical presentation of the patient after herpes zoster infection as back pain with referred leg pain, disc degeneration on MRI, intraoperative evidence of chronic neuropathy and almost complete improvement in patient symptoms after radiofrequency ablation makes it a first reported case of sinuvertebral neuropathy following herpes zoster infection.
INTRODUCTION
Varicella-Zoster virus is a neurotropic virus of the herpes virus family that primarily affects sensory nerves [10]. We present here a case of a herpes zoster infection in 55 years old man causing sinuvertebral neuropathy. To the best of our knowledge, no article has described the association of herpes zoster infection with sinuvertebral neuropathy and its successful treatment using percutaneous endoscopic radiofrequency ablation using interlaminar approach.
CASE REPORT
A 55 years old man presented with low back pain, both buttocks, posterior thigh and leg pain over last 3 months. A straight leg raising test was positive on both sides. A left great toe dorsiflexion was decreased to 4/5. The visual analog scale score at admission for back and leg pain was 7/10. There was still hyperpigmentation of skin characteristics of old herpes zoster infection on the back, right buttock and thigh (Fig. 1). The patient was on antiviral medications when he initially developed the skin lesions before 3 months. Then he started on steroid and gabapentin but there was no improvement in back, buttock, thigh and leg pain. He also had the twice epidural neuroplasty but no improvement. The patient MRI was showing disc degeneration at L5-S1 level (Fig. 2A). Owing to severe pain refractory to conservative management, we decided to do annuloplasty using structural preservation percutaneous endoscopic lumbar interlaminar approach [13] on the left side under epidural anaesthesia (Fig. 2B). We used an endoscope system with a 30-degree viewing angle, 7.3 mm outer diameter, and 4.7 mm working channel (Joimax GmbH, Karlsruhe, Germany). The entire operation was performed under visual control and continuous irrigation with normal saline (0.9%). There was severe vascularization in the midline and contralateral side (Fig. 3; Video 1) which was suggestive of sinuvertebral neuropathy [11]. We performed annuloplasty using radiofrequency ablation (Ellman’s bipolar radiofrequency electrocoagulator - Elliquence, Baldwin, New York, USA) to denervate the sinuvertebral nerve attached to the annulus. Radiofrequency ablation performed on the ipsilateral side over the contained disc and almost upto the contralateral foramen and dorsal root ganglion (Fig. 3). Patient symptoms completely relieved at the postoperative period and continued upto recent follow up of 6 months. The hyperpigmentation also improved significantly over the period of time (Fig. 1).

Clinical picture showing the improvement in skin lesions over period of time Ⓐ. Immediate post-op Ⓑ at one month follow up and Ⓒ at three months follow up.
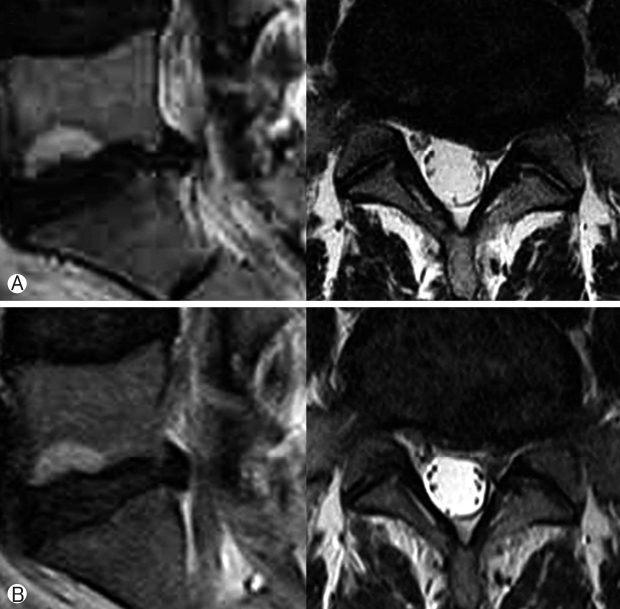
Ⓐ Preoperative T2-weighted MRI image of the L5-S1 level showing disc degeneration; Ⓑ Postoperative MRI after annuloplasty.
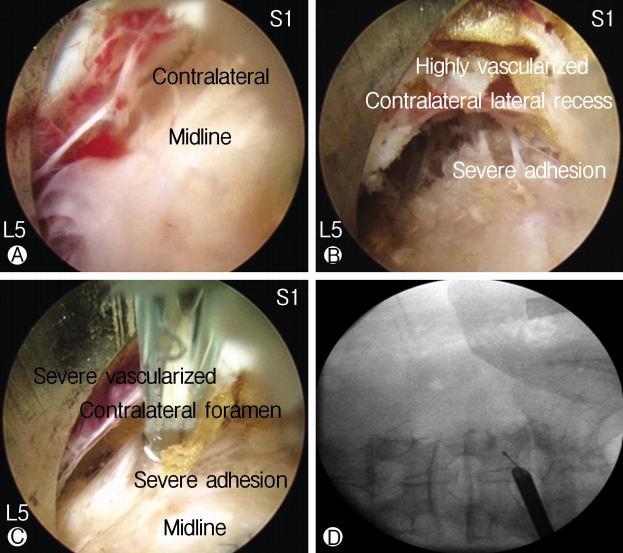
Intraoperative images showing severe vascularization and adhesions in the midline Ⓐ, a contralateral lateral recess Ⓑ and contralateral foraminal area Ⓒ. C arm image Ⓓ showing the position of the tip of the radiofrequency probe and working channel while doing adhesiolysis and annuloplasty as shown in image Ⓒ.
DISCUSSION
Herpes zoster is a viral disease occurs due to reactivation of the highly contagious varicella-zoster virus. During primary infection, the virus gains entry and persists in the sensory dorsal root ganglion. Reactivation of the varicella-zoster virus occurs due to depression of cell-mediated immunity and in aged patients [16]. The thoracic dermatomes are affected in 50-56%. The head area including trigeminal and other cranial nerves (VII and VIII) in 20% [7]. Rarely the virus affects cervical, lumbar and sacral segments [6]. The exact incidence of herpes zoster affecting the lumbar spine is not mentioned in the available literature.
Herpes zoster neuralgia should be considered in differential diagnosis of sciatica, as early treatment is of prime importance to avoid long-term neurological complications [2,8]. The treatment of herpes zoster includes pain management and antiviral medications. The neuralgic pain is treated in a stepwise manner using WHO analgesic ladder. The radiculopathy associated with herpes zoster can be treated with selective nerve root block or epidural neurolysis [5,9,20]. An antiviral treatment should be administered within 48-72 hours after the onset of clinical features. It can be either oral or intravenous [2].
Indications for an antiviral therapy include:
• Age more than 50 years,
• Immunocompromised status,
• severe zoster of the trunk or extremities,
• zoster of the head, neck or sacral area, and
• severe dermatitis [7].
This antiviral drug needs to be given for a minimum of 7 days.
Postherpetic neuralgia (PHN) is a chronic neuropathic pain after the herpes zoster (HZ) infection and persists even after the cutaneous lesions have healed. Despite various treatment advances, many patients remain noncompliant to the current therapies and continue to have pain; physical and psychosomatic distress [21]. In our case, the patient received the complete course of antiviral drugs after he developed the dermatological manifestations. Due to persistent and painful sinuvertebral neuropathy, he visited us after 3 months of diagnosis of herpes zoster.
The herpes virus infection is also one of the factors, which promotes disc degeneration [1]. Though the changes in lumbar spine morphology can be diagnosed using MRI, the precise location of the pain-inducing region cannot be distinguished [14,17,19].
Racz’s also known as “epidural neuroplasty” is minimal invasive epidural catheter procedure. Its principle of action is local epidural lysis of adhesions, neurolysis of spinal nerve roots, and local lavage of proinflammatory mediators by repeated injections of local anesthetics, corticosteroids, hyaluronidase, and hypertonic saline solution [22]. We performed this procedure twice but there was no improvement in pain which diminished the possibility of radiculopathy.
The sinuvertebral nerves arise in the intervertebral foramina from 2 roots, 1 from the ventral primary ramus and the other from a ramus communicans (Fig. 4A) [12]. These nerves are implicated in diffuse low back pain because of their pathway and its sympathetic component. Pain impulses coming from the intervertebral disk, posterior longitudinal ligament, and ventral part of the dura join the L2 spinal ganglion (somatic system) via the rami communicantes and sympathetic trunk. Therefore the sinuvertebral nerve as a carrier of deep somatic pain is related to referred pain and exhibits similar pain characteristics as radicular pain. Chronic derangement of the sinuvertebral nerve can induce neural degeneration, infiltration of neural tissue into the intradiscal space, and aggravation of disk degeneration (Figs. 4 and 5) [18].
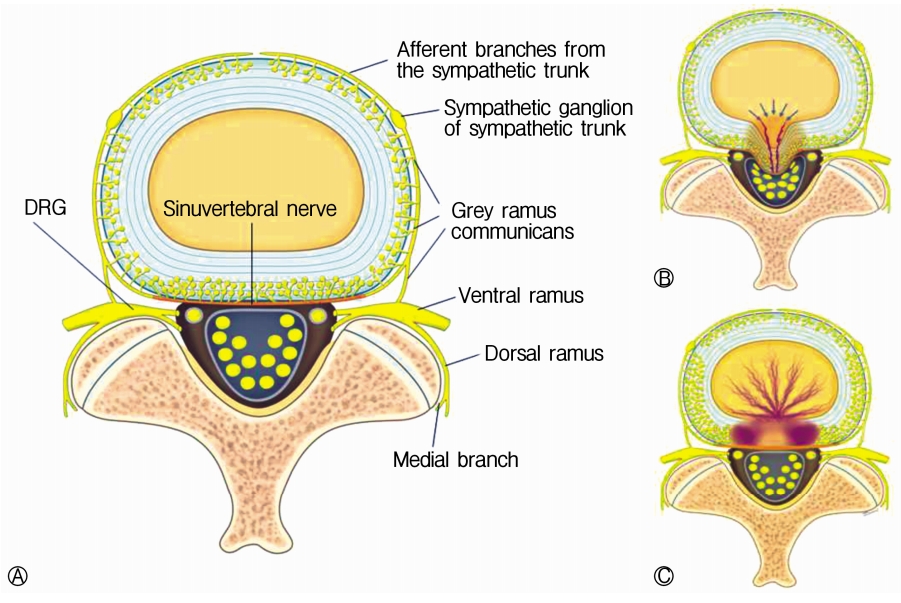
Schematic diagram of an axial section of the spine showing. Ⓐ Anatomy of the sinuvertebral nerve, normal state; Ⓑ Disc degeneration with an annular tear; Ⓒ Pathologic state where nerve grows inside the disc and gets sensitized around the posterior annulus and posterior longitudinal ligament.
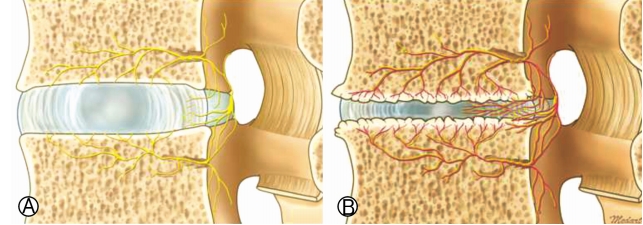
Schematic diagram of sagittal section of spine showing. Ⓐ Anatomy of the sinuvertebral nerve ‘s’ and basivertebral nerve ‘b’ - normal state; Ⓑ Pathologic state where nerve grows inside the disc and gets sensitized around the posterior annulus and posterior longitudinal ligament.
The endoscopic ablation of sinuvertebral nerve resulted in almost complete improvement in patient symptoms. The endoscopic interlaminar approach is the most minimally invasive approach to diagnose and treat sinuvertebral neuropathy for the L5-S1 level. Transforaminal access is difficult for L5-S1 level since, the highest part of the iliac crest is located above the L5-S1 level, making it difficult to access the L5-S1 disk space [3,4,15]. In addition, the L5 transverse process is the largest among the lower vertebral bodies and bends downward [12]. The sacral ala is also responsible for narrowing the L5-S1 intervertebral foramen.
The classical presentation of the patient after herpes zoster infection as back pain with referred leg pain, disc degeneration on MRI, intraoperative evidence of chronic neuropathy and almost complete improvement in patient symptoms after radiofrequency ablation makes it a first reported case of sinuvertebral neuropathy following herpes zoster infection.
CONCLUSION
The possibility of sinuvertebral neuropathy must be kept in mind as a sequel to herpes zoster, which mimics as lumbar radiculopathy. A percutaneous endoscopy is a powerful tool in diagnosis and management of this rare scenario. Early diagnosis and treatment of this condition are of the essence to improve outcome.
Notes
Financial Disclosure
No funds were received in support of this work.
No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.
Supplementary Material
Video 1.
Short Intraoperative video.