INTRODUCTION
Many case reports of various types of degenerative cysts are available [3,4,7]. These cysts can surprise surgeons with their appearance and place a diagnostic challenge both preoperatively and intraoperatively. We report a case of degenerative intraspinal cyst with severe adhesion to dura, which mimicked a nerve root and created a diagnostic dilemma during surgery.
CASE DESCRIPTION
A 60-year-old man presented to our clinic with insidious onset, gradually progressive lower back pain, right leg pain and neurological claudication of six months duration. The pain was radiating to the right S1 dermatome. Visual analogue score (VAS) for pain was 8.
On examination, patient had a positive straight leg raise test at 45 degrees on the right side. His sensation diminished on the right L5 and S1 dermatomes. However, the patient had no motor weakness.
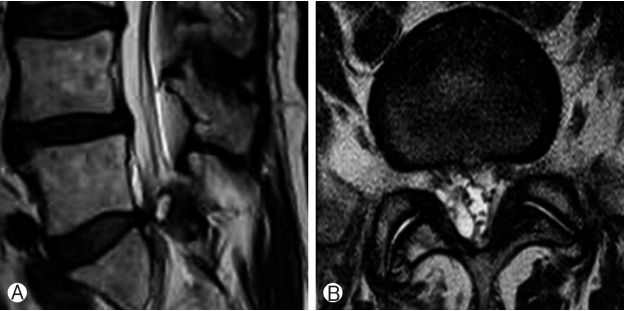
Magnetic resonance imaging (MRI) of the patient showed a large cystic lesion at right L5-S1 level. The cyst was compressing the dural sac and traversing right S1 root at L5-S1 level. The lesion was isointense on T1-weighted images and hyperintense on T2-weighted images (Fig. 1).
A diagnosis of right sided intraspinal cyst at L5-S1 level with neurological compromise was made.
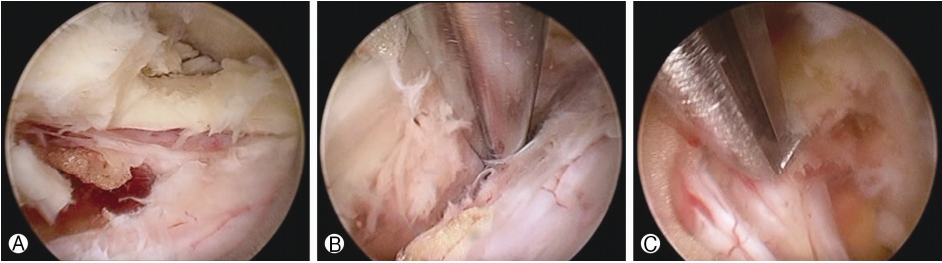
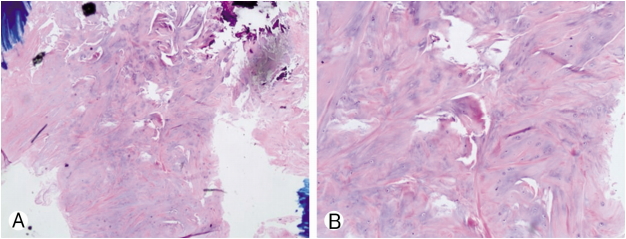
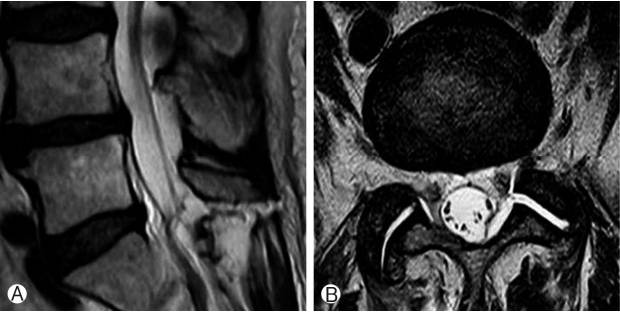
The patient was treated at our hospital using uniportal full endoscopic technique. Intraoperatively, the cyst appeared as nerve root and due to adhesions between dura and cyst meticulous dissection was required to identify and separate the cyst from neural structures (Fig. 2 & Video). Patient’s symptoms improved significantly after surgery and visual analogue score (VAS) of the patient was 2. At six months follow up he was faring well and asymptomatic. Histology confirmed the diagnosis of degenerative intraspinal cyst (Fig. 3). Post-operative MRI showed removal of the cyst and decompression (Fig. 4).
DISCUSSION
In the literature, various types of cysts have been described in the lumbar canal [4,6,7]. These cysts are classified according to anatomical location (such as facet cysts or ligamentum flavum cysts) or pathology (such as synovial or ganglion cysts) [1,3,7]. Usual presentation of the spinal canal cysts are low back pain, claudication, radicular pain, motor weakness, dysasthesia all of which are secondary to the compression of the neural elements or narrowing of the canal [2,4,7]. Neuroimaging modalities like myelography, computed tomography and MRI are helpful in the diagnosis of the spinal canal cysts [1,7]. Fibrous, collagenous and myxoid degeneration may be found on histological studies. In addition chronic granulomatous tissue, calcification, hemosiderin deposits may also be present [2,4,7]. Histopathology in our case confirmed degenerative intraspinal cyst.
Surgical excision followed by histopathological studies is the preferred treatment [4,7]. We performed the excision of the cyst with uniportal full endoscopic technique. Intraoperatively, we found a structure in right lateral recess which appeared as a nerve root and on further dissection came out to be the cyst we were looking for (Fig. 2 & Video 1). We used full endoscopic approach in this patient because interlaminar approach endoscopic surgery has already been established as a surgical option for spinal stenosis [5]. For that reason we decided to excise the cyst with full endoscopic surgery but due to adhesions the task became difficult as described above. We used interlaminar PESLD (Percutaneous Endoscopic Stenosis Lumbar Decompression) method described first by Kim et al. [5]. With meticulous dissection using probe we confirmed that the structure appearing as root actually was a cyst. Careful dissection through adhesions was the key to success of the full endoscopic removal of the cyst.
As can be seen from this report, a cyst appearing as a nerve root is a diagnostic dilemma and surgical challenge. In endoscopic surgery utmost care is needed to recognize the neural and other vital elements lest they get violated inadvertently during the procedure.
CONCLUSION
It is not common for a cystic lesion to masquerade as nerve root. However, such a situation is a dilemma to the surgeon and poses a surgical challenge to identify the lesion correctly and save neural and other important structures. Furthermore, this case report opens another dimension to the surgical management of the intraspinal cyst with the usual advantages of the minimally invasive solution like interlaminar approach percutaneous full endoscopic lumbar stenosis lumbar decompression (PESLD).